
Heart valve disease presents one of the most challenging diagnostic areas in cardiology because timing of intervention is critical – too early and patients undergo unnecessary procedures, too late and irreversible heart damage may occur. Dr Cassar’s triple accreditation in cardiac imaging (echocardiography, cardiac MRI, and cardiac CT) provides the comprehensive assessment needed to make these crucial timing decisions accurately.
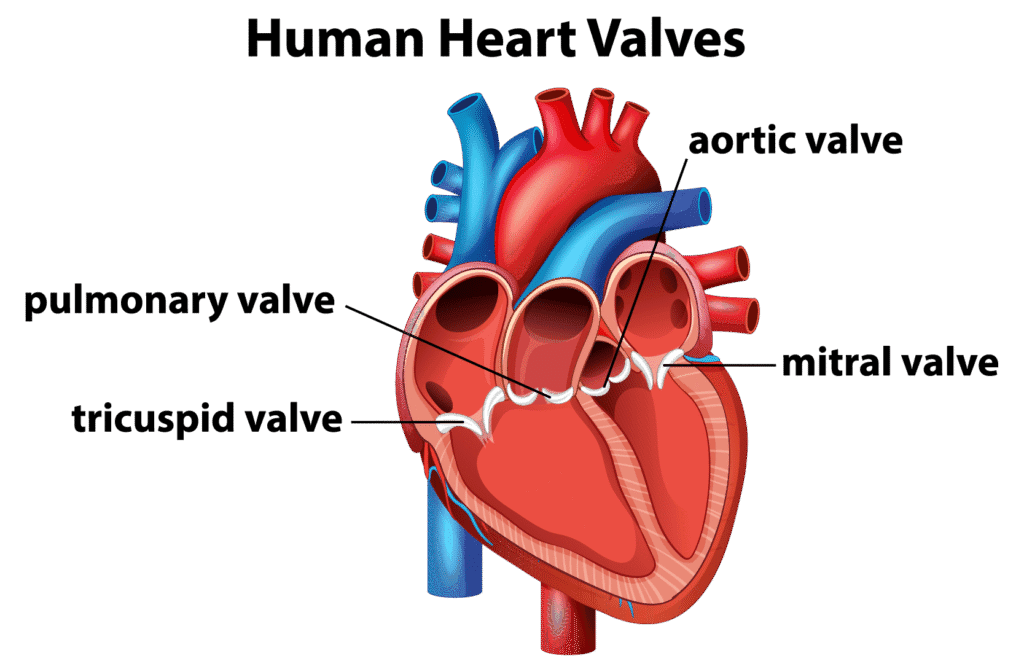
The heart has four valves: two on the right (tricuspid and pulmonary) and two on the left (mitral and aortic). When valves function normally, they allow unopposed forward flow of blood, while also preventing backward flow. These valves can either narrow (stenosis) or leak (regurgitation). In both scenarios, the heart has to pump harder to transport blood to the lungs and the other organs. Some valve problems develop slowly over decades, whilst others can deteriorate rapidly. The challenge lies not just in detecting valve disease, but in determining its impact on the heart (haemodynamic significance) and optimal management timing.
Valve disease severity cannot be assessed by symptoms alone. Many patients with severe valve disease feel relatively well for a long time before problems develop, whilst others experience significant symptoms with only moderate disease. This is why expert cardiac imaging, in combination with careful history taking and physical examination, is essential.
Valve disease symptoms can be subtle. Breathlessness is the most common symptom, initially occurring only with exertion but potentially progressing to affect rest or sleep as disease worsens. Many patients don’t recognise gradual decline because they subconsciously reduce activity levels – something careful history-taking can reveal. Chest tightness can occur, particularly with aortic stenosis, though severe valve disease can exist without chest pain. Palpitations can indicate atrial fibrillation, a common complication of mitral valve disease.
Some patients present with more alarming symptoms: blackouts are concerning for severe aortic stenosis, whilst fluid retention and leg swelling may be a sign that the heart is not coping. However, Dr Cassar emphasises that symptom severity doesn’t always correlate with disease severity. Some people with severe valve disease report little symptoms, whilst others feel quite unwell with moderate disease. This unpredictable relationship between the severity of symptoms and severity of the valve disease underscores why quantitative imaging assessment is crucial; treatment decisions cannot be based on symptoms alone.
Particularly during physical activity or when lying flat
Feeling unusually tired even with normal activities
Pressure or tightness in the chest, especially with exertion
Light-headedness or loss of consciousness
Awareness of irregular or rapid heartbeat
Fluid retention in the feet, ankles, or legs
Diagnosing valve disease accurately requires combining what’s heard during examination with detailed imaging measurements. Heart murmurs -abnormal sounds heard through a stethoscope – provide important clues about which valve might be affected. However, the loudness of a murmur does not necessarily represent the severity of valve disease; some severe valve problems produce quiet murmurs, whilst some innocent murmurs sound quite dramatic. This is why Dr Cassar always confirms examination findings with imaging rather than relying on clinical assessment alone.
Understanding what might have caused valve disease is also important. Previous rheumatic fever (which is now rare in the UK but still relevant for some patients), a history of heart valve infections, connective tissue conditions like Marfan syndrome, or previous chest radiotherapy can all damage heart valves. Family history is also taken into consideration – conditions like bicuspid aortic valve (where the aortic valve has two cusps instead of three) and mitral valve prolapse can run in families.
Dr Cassar develops personalized treatment plans based on the severity of your heart valve disease, your symptoms, and your overall health goals. Treatment approaches may include:
Medical therapy for valve disease has important limitations; medications can’t fix a damaged valve, but they can treat consequences and complications. Blood pressure control is very important in aortic regurgitation, to reduce the back-pressure on the heart (which in turn results in less blood flowing in the wrong direction). Water tablets (diuretics) reduce water retention symptoms when heart failure develops. Blood thinners may be needed if atrial fibrillation complicates mitral valve disease. Medications that slow the heart rate (such as beta blockers) improve symptoms when a fast heart rate (tachycardia) impacts heart and valve function.
Although very helpful, Dr Cassar emphasises that medical therapy isn’t a substitute for timely intervention when valve disease becomes severe. The key question is often not “what medications should I take?” but rather “will I need valve intervention?”, and if so “when is the right time for valve intervention?” This requires serial imaging to assess not only if the valve disease is progressing, but also whether the heart is coping well enough. Guidelines provide thresholds for intervention, but individual decisions consider age, symptoms, heart function, other health conditions, and patient preferences.
A common question patients ask is whether lifestyle changes can improve their valve problem. The honest answer is that whilst lifestyle modifications cannot repair a damaged valve, they can help you feel better and reduce strain on your heart whilst the valve disease is being monitored or awaiting treatment.
Maintaining a healthy weight makes a real difference – excess weight forces your heart to work harder, which becomes particularly problematic when a valve isn’t functioning properly. If you’re experiencing breathlessness or leg swelling, reducing salt intake can help minimize fluid retention and improve symptoms. Blood pressure control is especially important, as high blood pressure adds extra stress to an already struggling valve.
Exercise is generally beneficial, but the appropriate level depends on your specific valve problem and its severity. Many patients with mild to moderate valve disease can continue regular activities and exercise normally. However, if you have severe aortic stenosis, strenuous exertion should be avoided – Dr Cassar provides tailored advice based on your individual situation, ensuring you know what’s safe and what to avoid.
Patients often ask about supplements, vitamins, or alternative therapies for valve disease. Unfortunately, no dietary supplement can reverse structural valve damage or improve valve function – this is one area where the scientific evidence is clear. However, standard cardiovascular health measures do matter: managing cholesterol, keeping diabetes well-controlled if you have it, and stopping smoking all protect your heart muscle from additional stress. These measures won’t fix the valve, but they optimize the rest of your cardiovascular system whilst you’re living with valve disease.
For severe aortic stenosis, once symptoms develop, prognosis without intervention is poor – this is one scenario where intervention timing is relatively straightforward. Mitral regurgitation presents more complex decisions: intervention before irreversible heart damage occurs is ideal, but operating too early exposes patients to unnecessary procedural risk. Dr Cassar’s experience and detailed imaging assessment identifies the right timing by tracking the size and function of the heart, as well as the severity of the valve problem, over time.
Modern valve interventions range from open surgical repair or replacement to minimally invasive and transcatheter (keyhole) procedures. TAVI (transcatheter aortic valve implantation) involves inserting a new valve through a catheter, usually via an artery in the groin, without needing open heart surgery. This has transformed treatment for older patients or those where open heart surgery poses too high a risk. Similarly, for mitral and tricuspid valve leaks, edge-to-edge repair offers a minimally invasive option—a clip is placed via catheter to bring the valve leaflets together, reducing the leak without open surgery. Although this is an attractive and minimally invasive solution, surgery (particularly valve repair) remains superior to clip procedures in most patients.
Dr Cassar’s pre-procedural imaging assessment—particularly transoesophageal echocardiography (TOE) and cardiac CT—provides surgeons and interventional structural cardiologists with detailed anatomical information. This imaging guides procedural planning, determines whether a patient is suitable for minimally invasive approaches, and helps select the right prosthetic valve size and type.
Dr Cassar works with specialist valve surgeons and structural interventional cardiologists at tertiary centres, maintaining involvement throughout the treatment pathway. This includes optimizing imaging before procedures, coordinating referral to appropriate specialists, and providing post-procedural follow-up with regular imaging to monitor valve function. This integrated approach means patients benefit from specialist intervention whilst maintaining their ongoing relationship with Dr Cassar for cardiac care.
Valve disease requires regular monitoring because it progresses at different rates in different people. Medical guidelines recommend follow-up intervals based on how severe the valve problem is, but these are averages – some patients deteriorate quickly whilst others remain stable for many years. Dr Cassar uses the same imaging techniques at each visit, making it possible to spot meaningful changes over time. Small changes in measurements – such as how narrow a valve is becoming, how much it’s leaking, or whether the heart chambers are enlarging – can signal that the valve disease is worsening and may need treatment sooner rather than later.
If you’ve had valve surgery or a TAVI procedure, ongoing check-ups remain important. Replacement valves need monitoring to ensure they’re working properly and haven’t developed problems like leaks around the edges or blood clots. Tissue valves (bioprosthetic valves) typically last 10-15 years, so younger patients may eventually need another procedure – regular imaging helps detect valve wear before problems become serious. After surgical repair, monitoring confirms the repair is holding up well.
Having access to multiple imaging techniques offers important advantages. If ultrasound scans become difficult (which can happen due to body shape, lung disease, or previous surgery), cardiac MRI provides clear images instead. If one test gives unclear results about how a replacement valve is functioning, another technique can provide the answer. This flexibility means you receive accurate monitoring regardless of technical challenges, ensuring valve problems are detected and managed at the right time.
Aortic stenosis is the most common heart valve problem in the UK, particularly in older adults. This happens when the aortic valve becomes narrow and stiff, making it harder for blood to flow from your heart to the rest of your body. Another common condition is mitral regurgitation, where the mitral valve doesn’t close properly and allows blood to leak backwards. Every patient’s valve problem is different, which is why detailed heart scans are essential to understand exactly what’s happening with your valve and how best to treat it.
How serious valve disease is depends on which valve is affected, how badly it’s damaged, and whether it’s getting worse over time. Mild valve problems may only need monitoring with regular check-ups, whilst severe valve disease can lead to serious heart problems if not treated. The good news is that many people with valve disease live normal, active lives with the right monitoring and treatment. Regular heart scans help track your valve and ensure any treatment is given at the best time for you, before complications develop.
Valve disease itself cannot be cured with tablets alone, but it can be successfully treated. If your valve disease is mild, it can be monitored carefully with regular check-ups and scans, along with simple lifestyle changes to keep your heart healthy. When valve disease becomes more severe, valve surgery can fix or replace the damaged valve, allowing your heart to work normally again and helping you feel much better. Modern keyhole surgery techniques include TAVI (where a new valve is inserted through a blood vessel, typically the leg, without opening the chest) for aortic stenosis, and edge-to-edge repair (a clip procedure to fix leaky valves) for mitral regurgitation and tricuspid regurgitation. These minimally invasive procedures have excellent success rates and much quicker recovery than traditional open-heart surgery. The most important thing is catching valve problems early through expert assessment, so treatment can be given at exactly the right time.
Some types of valve disease can run in families. Bicuspid aortic valve (where the valve has two flaps instead of the normal three) is often inherited, as are certain conditions affecting the body’s connective tissues that can weaken valves. However, most valve disease develops over time due to age-related wear and tear, past infections like rheumatic fever, or other causes. If you have valve disease, it’s worth mentioning this to close family members, particularly if you have a bicuspid valve or a connective tissue condition, as they might benefit from being checked too.
Yes, valve disease is often first spotted during a routine check-up when your GP hears an unusual heart sound called a murmur using a stethoscope. Murmurs are caused by rough blood flow through a narrowed or leaky valve. Not all murmurs mean valve disease – some are harmless – but any new murmur should be checked with a heart scan (echocardiogram). This is why regular check-ups are so important. Some people have valve disease for years without knowing because they’ve gradually slowed down without realizing it and don’t have obvious symptoms. If a murmur is found, you’ll be referred to a heart specialist like Dr Cassar for a detailed assessment using advanced heart scanning.
Important warning signs include becoming more breathless, especially during activities you used to manage easily, new chest discomfort or tightness, feeling dizzy or faint, noticing your heart racing or beating irregularly, or swelling in your ankles and legs. If you find yourself getting unusually tired or needing to rest more often during daily activities, this could mean your valve problem is progressing. Any sudden worsening of these symptoms needs urgent medical attention. Regular monitoring appointments help spot changes in your valve before symptoms become severe.
How often you need appointments depends on how severe your valve problem is and whether you have symptoms. Mild valve disease usually needs checking every 3-5 years, moderate disease every 1-2 years, and severe disease every 6-12 months or more often if symptoms change. Dr Cassar uses advanced heart scans—ultrasound, MRI, and CT—to track your valve accurately over time. If you notice any new symptoms between appointments, you should be seen sooner. Regular monitoring ensures any treatment is timed right for the best outcome.
Most people with mild to moderate valve disease can exercise safely and should stay active. What type of exercise and how hard you can push yourself depends on which valve is affected and how severe the problem is. Dr Cassar provides personalized advice based on your specific condition, sometimes including an exercise test to work out safe activity levels for you. Staying physically active is generally good for your heart health, though very intensive competitive sports might need to be avoided in some cases. Your treatment plan will include clear guidance about exercise and what activities are safe for you.
What you should avoid depends on the type and severity of your valve problem. Most people with mild to moderate valve disease can continue all their normal daily activities without any restrictions, including housework, shopping, walking, and gentle gardening. You should generally avoid very hard physical work like heavy lifting, very intense exercise, or competitive sports if you have moderate to severe disease. Exercises where you’re straining hard (like lifting very heavy weights or pushing/pulling heavy furniture) can put extra pressure on your heart and are often best avoided. Dr Cassar will give you personal advice based on your specific condition, sometimes including an exercise test to work out what’s safe for you. The good news is that staying active within your limits is good for your heart and overall health.
Many people with valve disease live long, healthy lives with proper monitoring and treatment. How long you can live depends on which valve is affected, how bad the problem is, and whether you get the right treatment at the right time. Mild valve disease may never get worse and might only need regular check-ups throughout your life. For more severe valve disease, surgery works extremely well – studies show that 80-90% of patients who have valve replacement surgery for severe aortic stenosis are still alive five years later, compared to much worse outcomes without surgery. The key is having regular check-ups so that any treatment can be planned at exactly the right time, giving you the best possible long-term outcome.
Untreated severe valve disease can lead to serious problems. Your heart may become too weak to pump blood properly (heart failure), you may develop dangerous irregular heart rhythms, blood clots can form which might cause a stroke, and the heart muscle itself can become permanently damaged. This is why regular monitoring is so important – it allows treatment to be timed perfectly, before any lasting damage occurs. With proper check-ups and treatment when needed, these complications can usually be prevented.
Valve repair means fixing your own valve – for example, tightening a leaky valve or trimming away excess tissue so it closes properly. Valve replacement means removing the damaged valve completely and putting in an artificial one. Artificial valves can be mechanical (made from metal and specially treated carbon) or biological (made from specially treated animal tissue, usually from cows or pigs). Doctors prefer to repair your valve when possible because you keep your own natural valve, but replacement may be needed if the valve is too badly damaged. Dr Cassar works with expert heart surgeons to decide the best approach for your situation.
Both procedures replace a damaged aortic valve with a new one and have excellent success rates. The main difference is how the new valve is put in. Traditional surgery involves an incision in the chest to access and remove the old valve directly, then place a new one. TAVI is a keyhole procedure where a new valve is inserted through a small puncture in a blood vessel, usually in the groin, and expanded in position – this pushes aside the old valve. TAVI patients typically go home within 1-3 days and recover within a few weeks, whilst traditional surgery requires about a week in hospital and 6-8 weeks recovery time. Traditional surgery has decades of proven long-term results, whilst TAVI is a newer technique with excellent outcomes but less long-term data beyond 10-15 years. TAVI is often preferred for older patients or those with other health conditions, whilst traditional surgery may be better for younger patients who need a valve that will last many decades.
This depends on what type of valve and procedure you have. If you have a mechanical valve replacement, you’ll need lifelong blood thinning medication (warfarin) to prevent blood clots forming on the valve. Biological valves usually only need blood thinners for 3-6 months after surgery. Valve repair might need short-term blood thinners or sometimes none at all. If you develop an irregular heart rhythm called atrial fibrillation, you may need blood thinners regardless of which valve procedure you had. Dr Cassar will give you clear information about what medications you’ll need based on your specific treatment.
Recovery time varies a lot depending on what type of surgery you have. For traditional open-chest surgery, expect 6-8 weeks before getting back to most normal activities and 3-6 months for full recovery. You’ll typically be in hospital for 5-7 days. For keyhole procedures like TAVI (where the new valve is put in through a blood vessel) or edge-to-edge repair (a clip procedure to fix leaky valves), recovery is much faster – many patients go home within 1-3 days and get back to normal activities within 2-3 weeks. How quickly you recover also depends on your age, how fit you were before surgery, and whether you have other health problems. Most people notice their symptoms are much better soon after successful valve surgery. Dr Cassar works closely with experienced heart surgeons who will discuss expected recovery times for your specific operation.
Most patients can start driving again 4-6 weeks after traditional open-chest valve surgery, once your breastbone has healed enough. You must not drive while taking strong painkillers that might affect your ability to concentrate or react quickly. For keyhole procedures like TAVI or the clip procedure, recovery is much quicker and you may be able to drive within 1-2 weeks. You’re legally required to tell the DVLA about your heart surgery – they’ll tell you when you can start driving again. Your car insurance company should also be told. Dr Cassar will advise you on the specific timeframe for your type of surgery and will give you the all-clear when it’s safe for you to drive again.
Current guidelines say you only need antibiotics before dental procedures in specific high-risk situations. You’ll need them if you have an artificial heart valve, if you’ve previously had a heart valve infection, certain types of heart problems you were born with, or if you’ve had a heart transplant with valve issues. Most people with valve disease—even quite severe valve disease – do not need antibiotics before routine dental work. However, good dental hygiene and regular dental check-ups are important for everyone with valve disease, as gum infections can potentially spread to the heart. Dr Cassar can tell you specifically whether you need antibiotics before dental treatment based on your situation.
This depends on what type of valve disease you have. If you have a bicuspid aortic valve (where the valve has two flaps instead of the normal three), your children have a higher chance of having it too and should have a heart scan to check, as this often runs in families. Similarly, if you have an inherited condition affecting connective tissues in your body that has damaged your valves, family screening is important. However, if your valve disease is due to age-related wear and tear or other causes you weren’t born with, your family members don’t usually need routine screening. It’s worth discussing your family history with Dr Cassar, who can advise whether your relatives would benefit from being checked.
You should consider seeing a cardiologist like Dr Cassar if you’ve been told you have a heart murmur that needs investigation, if you’re experiencing symptoms like breathlessness, chest tightness, dizziness, or palpitations, if your valve disease is moderate or severe and you’re wondering about treatment options, if you need assessment for possible valve surgery or repair, or if you want a second opinion about your valve condition. Many patients are referred by their GP when valve disease is first detected or when it progresses to a stage requiring specialist input. Dr Cassar’s triple accreditation in cardiac imaging (echocardiography, MRI, and CT) means he can perform and interpret the most detailed heart scans himself during your consultation, providing immediate, expert assessment of your valve function. This level of imaging expertise is particularly valuable for determining the severity of valve disease, assessing whether it’s affecting your heart muscle, and deciding on the optimal timing for intervention. At his clinics in Basingstoke and Winchester, appointments are typically available within 1-2 weeks.
Whilst GPs can diagnose valve disease through examination and arrange basic tests, a specialist cardiologist like Dr Cassar provides expertise that’s crucial for managing valve conditions effectively. Dr Cassar’s advanced imaging skills allow for detailed assessment of valve structure and function that goes far beyond standard testing. He can accurately determine valve disease severity using multiple imaging techniques, detect early effects on your heart muscle before symptoms develop, assess whether you’re a candidate for valve repair versus replacement, coordinate your care pathway with leading cardiac surgeons at tertiary centres, and provide ongoing monitoring with the most advanced imaging available. For patients considering valve surgery, Dr Cassar’s assessment is essential for timing intervention appropriately—operating too early means unnecessary risk, but waiting too long can lead to irreversible heart damage. His extensive experience and imaging expertise ensure treatment decisions are made at exactly the right time for optimal outcomes.
Dr Cassar typically offers appointments within 1-2 weeks for valve disease assessment, providing prompt access whether you’re newly diagnosed, experiencing worsening symptoms, or seeking a second opinion about treatment options. The private clinic setting at Candover Clinic in Basingstoke ensures you’ll have Dr Cassar’s full attention during your consultation, with appointments typically lasting 30-45 minutes. Many patients can have echocardiography performed during their first visit, with Dr Cassar interpreting the images immediately rather than waiting weeks for a separate scan appointment. This comprehensive, same-visit approach means most patients leave their first appointment with a clear understanding of their valve disease severity, how it’s affecting their heart, and a detailed treatment plan.
There are excellent resources to support you in managing heart valve disease: