Why timing matters in heart valve disease
In heart valve disease, the main question is often not simply whether a valve is abnormal. It is whether the valve problem is severe enough to need treatment, and whether the heart is beginning to show strain.
Treating too early can expose a patient to unnecessary procedural risk. Waiting too long can allow irreversible heart muscle damage. The decision usually depends on symptoms, echocardiogram measurements, heart size, heart function and sometimes additional imaging.
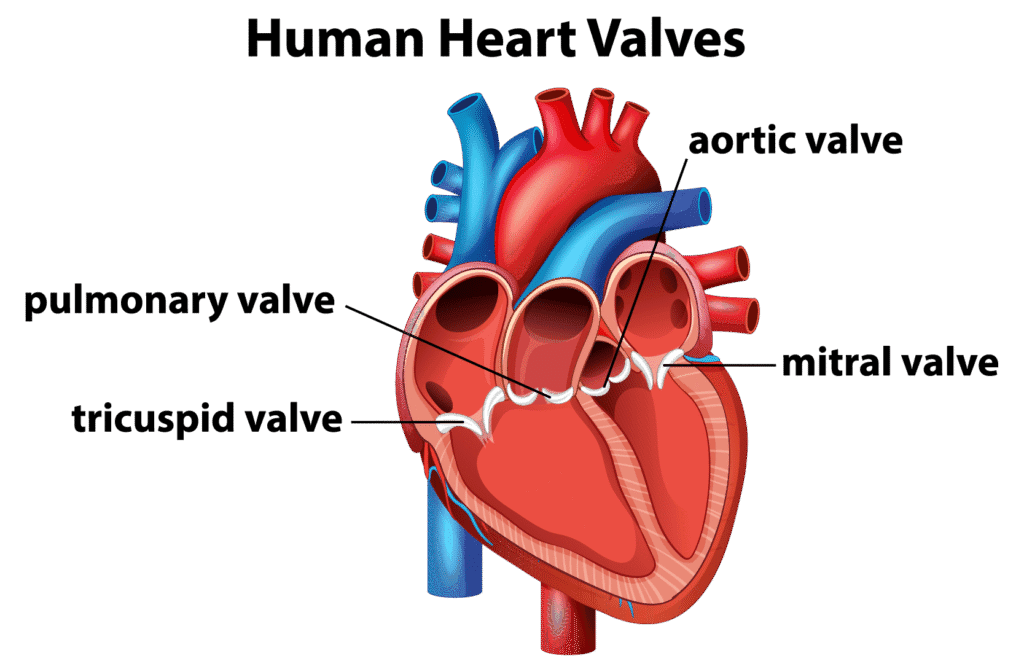
The common valve problems
The heart has four valves: aortic, mitral, tricuspid and pulmonary. The aortic and mitral valves are the most commonly discussed in adult valve disease.
Aortic stenosis means the aortic valve has narrowed. The heart has to pump against higher resistance. Over time, this can lead to thickening of the heart muscle, breathlessness, chest pain, fainting or heart failure.
Mitral regurgitation means the mitral valve leaks. Blood flows backwards into the left atrium, and the heart may compensate for years before symptoms develop. The challenge is identifying when the leak has started to affect the heart.
Symptoms are important, but not enough
Symptoms such as breathlessness, chest pain, fainting, ankle swelling or reduced exercise capacity matter. In severe aortic stenosis, new symptoms are particularly important and should be assessed promptly.
However, some patients adapt gradually and do not notice how much their exercise capacity has fallen. Others have severe valve disease before obvious symptoms appear. This is why surveillance imaging is central to valve care.
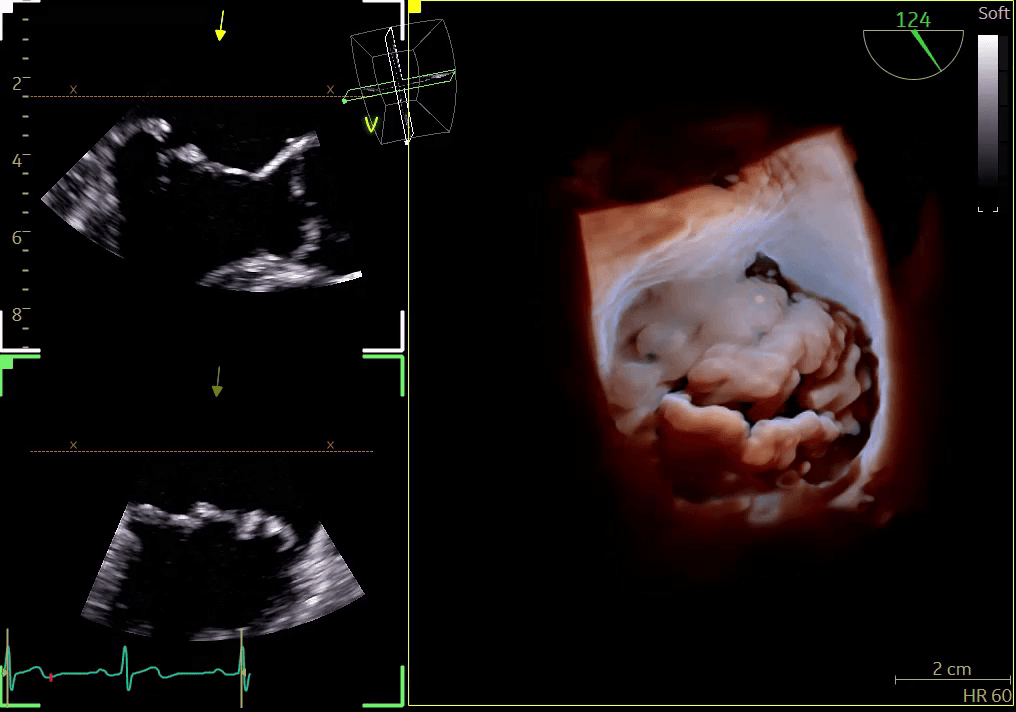
What echocardiography measures
An echocardiogram is usually the main test for valve disease. It can assess:
- how narrow or leaky the valve is;
- pressure gradients across the valve;
- the size of the heart chambers;
- left ventricular function;
- pulmonary pressures;
- whether the valve problem is affecting the rest of the heart.
These measurements help decide whether monitoring is enough, whether medication is relevant, or whether referral for valve intervention should be considered.
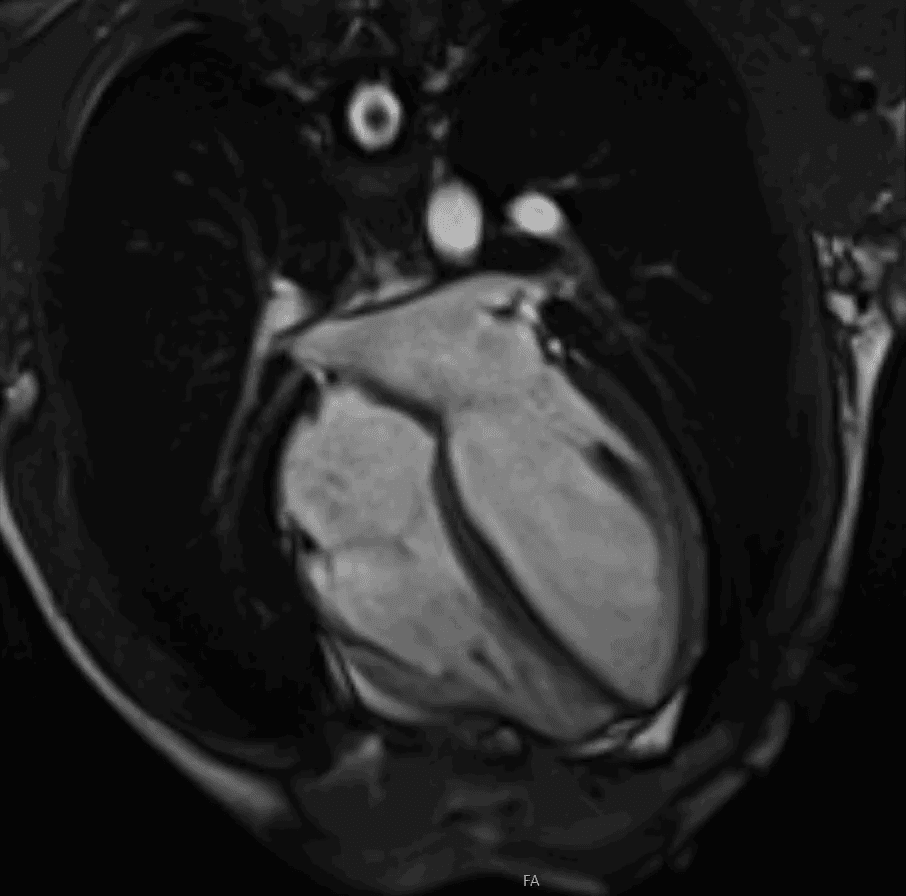
When CT or MRI may be needed
Echo is the starting point, but additional imaging can help in selected cases. Cardiac MRI can measure heart volumes and function very accurately and can help quantify some forms of valve leakage. Cardiac CT can define valve anatomy and is important in planning some procedures, including transcatheter aortic valve implantation.
Dr Cassar is accredited in echocardiography, cardiac CT and cardiac MRI. That is useful in valve disease because the decision is often made by combining information from more than one imaging test.
When to seek specialist valve assessment
Specialist assessment may be helpful if:
- you have been told you have a heart murmur but do not know the cause;
- you have known valve disease and have not had imaging recently;
- you have new breathlessness, chest pain, fainting or reduced exercise capacity;
- your echocardiogram describes moderate or severe valve disease;
- you have been advised that surgery or a transcatheter procedure may be needed;
- you want a second opinion on the timing of treatment.
For patients needing valve disease assessment with cardiac imaging, Dr Cassar sees patients at Candover Clinic and The Hampshire Clinic in Basingstoke, and The Berkshire Clinic in Reading. Details of available tests are on the cardiology services page, with booking information on the appointments page.